Delayed Delivery – Including Delayed Emergency C-Section – Can Cause Birth Injuries such as Hypoxic Ischemic Encephalopathy (HIE), Seizure Disorders & Cerebral Palsy

The birth of a baby is a joyous occasion, and in most cases, newborns are born healthy and do not require lengthy stays in the hospital. Sometimes, however, doctors and nurses fail to pay close attention to dangerous conditions in the mother and baby and they don’t pay proper attention to the fetal heart rate during labor and delivery. This carelessness often results in the medical team failing to promptly deliver the baby, which can cause the baby to be deprived of oxygen for too long. Prolonged oxygen deprivation can cause a baby to develop hypoxic ischemic encephalopathy (HIE), which can cause brain damage and conditions such as neonatal seizures, cerebral palsy, periventricular leukomalacia (PVL), motor disorders, hydrocephalus, developmental disabilities, intellectual disabilities and other birth injuries.
WHAT ARE PROLONGED & ARRESTED LABOR?
There are established timelines for what is considered a safe and normal progression of labor. If certain markers for labor progression (such as effacement and cervical dilation) are taking too long or are stalled, the healthcare team must appropriately evaluate the situation and decide if there is an arrest of labor. If there is an arrest of labor, or if the baby is in distress and is experiencing non-reassuring heart tones, the healthcare team may utilize different interventions to try and promptly deliver the baby vaginally. However, allowing labor to continue for too long increases risks for the baby, including oxygen deprivation and birth trauma. Thus, if early attempts to intervene do not result in timely delivery of the baby, healthcare professionals must be prepared to quickly move on to C-section delivery in order remove the baby from risky conditions and prevent significant oxygen deprivation and birth injuries such as HIE.
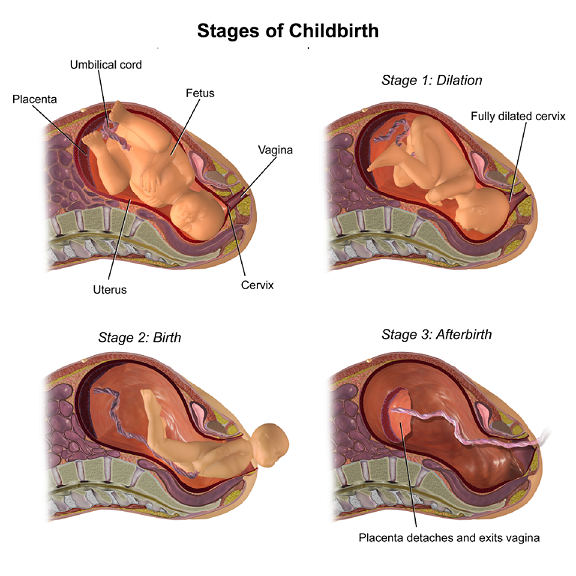
“Normal” labor occurs when contractions of the uterus cause progressive dilation and effacement of the cervix. The latent phase of labor typically progresses slowly. However, once there is cervical dilation of more than 4 centimeters (cm), the active or rapid phase of labor begins. In most cases, when the mother is in active labor, there should be progressive dilation of the cervix that occurs at a rate of no less than 1.2 cm per hour (for a mother’s first baby), or 1.5 cm per hour (for a mother’s subsequent babies). If the progression of labor occurs more slowly than this, the mother may be experiencing arrested labor, which is typically defined as an absence of progress (measured by dilation of the cervix and descent of the presenting part of the baby) for at least two hours. Often, doctors diagnose a mother with a “protracted active phase of labor” when she is at ≥ 6 cm dilation and is dilating less than about 1 to 2 cm per hour. Doctors often diagnose “active phase arrest” when the mother is at ≥ 6 cm cervical dilation with ruptured membranes and either no cervical change for ≥ 4 hours despite adequate contractions OR no cervical change for ≥ 6 hours with inadequate contractions.
Many doctors diagnose a prolonged second stage of labor when a nulliparous woman (a woman who has never given birth) without epidural anesthesia has pushed for 3 hours, or a multiparous woman (a woman who has experienced one or more previous childbirths) without epidural anesthesia has pushed for 2 hours, with an additional hour added for women receiving epidural anesthesia.
There are competing definitions of prolonged first and second stages of labor. Some research studies have found that labor is prolonged when the duration of the first and second stages of labor combined is > 20 hours for a first pregnancy and >14 hours for mothers who have previously given birth. Other experts define prolonged labor as a combined first and second stage of labor that occurs for 18-24 hours or more. Prolonged labor is more common in a first pregnancy and in women who are older than 35 years of age.
WHAT ARE THE CAUSES OF PROLONGED & ARRESTED LABOR, & WHEN IS A C-SECTION INDICATED?
Although many issues can cause prolonged and arrested labor, prolongation and arrest of labor are most often caused by mechanical impediments and / or inadequate contractions. Mechanical impediments include malpresentations (such as breech, face, brow, shoulder and asynclitic presentations) as well as cephalopelvic disproportion (CPD). Causes of CPD include an abnormally large baby (a macrosomic baby – which can occur when a mother has gestational diabetes), a baby with an abnormally large head (which can occur when the mother is past the due date or “post-term”), the mother has a clinically small pelvis, and / or there is malpresentation of the baby.
Inadequate uterine activity refers to uterine activity that is either not sufficiently strong or not appropriately coordinated to dilate the cervix and expel the baby.

Sometimes, the uterine muscle fails to contract properly when it is grossly stretched, which can occur when there is a twin pregnancy, or when the mother has a condition called hydramnios (excess amniotic fluid).
Insufficient contractions are often treated with uterine stimulation. Doctors often administer Cytotec or Pitocin (synthetic oxytocin) to stimulate the uterus. Too much of these drugs can cause uterine hyperstimulation, which can lead to cause oxygen deprivation in the baby; when contractions are too fast and strong, the placenta often cannot recharge with an adequate supply of oxygen-rich blood for the baby. As hyperstimulation continues, the baby can get progressively more oxygen deprived. Indeed, use of Cytotec or Pitocin requires very close monitoring of the baby’s heart rate; the baby must be quickly delivered at the first signs of distress.
Too much anesthesia or painkillers can cause inefficient uterine action and may prevent voluntary effort by the mother to deliver the baby during the second stage of labor. Research shows that anesthesia can increase the length of the second stage of labor.
BABIES MUST BE PROMPTLY DELIVERED – OFTEN BY EMERGENCY C-SECTION – WHEN THEY ARE IN DISTRESS
Regardless of whether the mother and baby are experiencing any of the aforementioned risky conditions – or any other risky labor and delivery issue – it is imperative that the baby be promptly delivered when there is fetal distress and fetal heart rate patterns that are concerning. Nonreassuring fetal heart tracings, including Category III tracings, require prompt delivery of the baby. Often, an emergency C-section is the safest and fastest way to deliver a baby in distress. Also, if a condition is present that is likely to cause significant distress, the baby may need to be urgently or emergently delivered. In addition, there are many conditions that require a C-section delivery, and it is important that doctors and nurses timely recognize this and plan accordingly.
Indeed, we have reviewed many cases in which a baby was in distress during labor and delivery and experiencing a risky condition, and the medical team failed to act with any sense of urgency in delivering the baby. This delay resulted in the baby being deprived of oxygen for too long and experiencing HIE and a brain injury. Sadly, in many of these cases, the prolonged oxygen deprivation, HIE and resultant brain injury could have been prevented with prompt performance of a C-section (often referred to as “emergency C-section”).
Prolonged oxygen deprivation (and ischemia) and hypoxic ischemic encephalopathy (HIE) can cause conditions such as neonatal seizures, cerebral palsy, motor disorders, periventricular leukomalacia (PVL), hydrocephalus, intellectual disabilities, developmental delays, and other long-term problems.
HYPOTHERMIA TREATMENT CAN MINIMIZE BRAIN INJURY & HELP PREVENT PERMANENT BRAIN DAMAGE IN NEWBORNS

There is a treatment that can minimize brain injury and help prevent permanent brain damage in babies: Newborns experiencing seizures and those who had low Apgar scores and/or abnormal umbilical cord blood gases – and those suspected of having HIE – can receive hypothermia (brain cooling) treatment, if certain criteria are met. It is negligence if the medical team fails to provide hypothermia treatment to a newborn who meets the criteria for this therapy.
THE MICHIGAN MEDICAL MALPRACTICE ATTORNEYS AT GREWAL LAW / CHURCH WYBLE P.C. ARE HERE TO HELP
If you think your baby experienced a traumatic birth, oxygen deprivation, a brain bleed, delayed delivery, or delayed emergency C-section, or if your baby’s care was mismanaged after birth in the NICU, please contact our team of experienced Michigan birth injury attorneys. The medical malpractice team at Grewal Law / Church Wyble P.C. is comprised of attorneys and healthcare professionals, including an on-site registered nurse, pharmacist, paramedic, and respiratory therapist. We also work with the best consultants from around the country, as well as a physician who has an office out our Okemos location. Our attorneys are licensed in Michigan and Florida, and we help victims of medical malpractice and birth trauma throughout Michigan and Florida.
If your baby was diagnosed with HIE, seizures, cerebral palsy, motor disorders, periventricular leukomalacia (PVL), hydrocephalus, intellectual disabilities, or developmental delays, or if you experienced problems during delivery or shortly before or after birth, please call us. Our medical malpractice attorneys and medical staff are available to speak with you 24/7.








